
 This post is part of our “Continuum of Care” blog series hosted by the Maternal Health Task Force
This post is part of our “Continuum of Care” blog series hosted by the Maternal Health Task Force
Esther has walked for 10 kilometers in the dusty red soil to her district health post in Mafinga, Iringa, Tanzania. She thinks she is pregnant; her belly is growing and her dada mkubwa (big sister) has said, “inaweza kuwa hivyo,” (it might be so) and she should go see a daktari (doctor).
She enters the clinic and there is a long queue. Over 30 women are waiting, some with their babies, growing impatient; they have to go back home to their chores or to the shambaa (field). She is told that the nurse-midwife only works until lunchtime because she has to go to the next village to give vaccines. The nurse-midwife tells Esther that she needs to do a test but can’t because they are out of stock. Maybe Esther can buy it at the local duka ya dawa (pharmacy)? She also tells Esther to come regularly to the clinic to have her belly, weight and blood pressure checked and make sure she takes her iron and folic acid tablets. But the clinic is only open three mornings a week, so Esther may have to come multiple times in order to be seen even once.
Overwhelmed, Esther wonders how she will manage over the next few months.
So what is the care Esther received? Some of the standard questions we use to assess this include:
- Did she go to care in her first trimester of pregnancy?
- Has she had her four antenatal check-ups?
- Was she attended by a skilled birth attendant?
To answer those questions, Esther would show the tablets she received, and say a doctor gave them to her because the provider wore a white coat. On any health-related census or household survey, Esther would be included as having received adequate care even though her care was far from adequate.
But have we really measured the quality of care she received?
To measure quality of care, we should ask Esther more detailed questions: whom she sees at the antenatal clinic and what is available there. Did she have access to vaccines, vitamins, antibiotics, and weighing scales? Did she feel she could easily access the antenatal services, with both the permission and monies to go? Were the services acceptable or respectful; did she feel she could ask any questions or be seen in privacy? Was it comprehensive antenatal care she received? Was she reassured during her pregnancy and counseled on what to expect and how to deal with emergencies? Was she advised where to have her baby and did she feel that she can visit the clinic at any time?
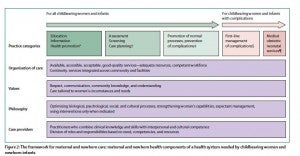
In the Lancet series on Midwifery, we started our discussion and research from the perspective of what women and newborns need. We knew without evidence there is no basis for change. We also knew that for all women—including those like Esther—sexual, reproductive, maternal, and neonatal health (SRMNH) services need to shift from fragmented care to integrated care. The series shows that this care should be provided by a team of educated, regulated health care professionals working in an enabled health system delivering quality maternal and newborn care (QMNC). QMNC incorporates not only what type of care is delivered, but also how its organized and delivered. This includes quality care practices and optimising normal processes and using interventions only when indicated while showing respect for women and tailoring care to their needs. We developed a framework that brings this all together:
QMNC Framework
What does this mean for the care providers?
Care providers are hard put to deliver quality care outside an enabled environment. If you cannot provide the health care women need, communicate with colleagues, or refer women with complications, at some point you’re going to hit a wall. The QMNC framework can help health workers better define which care to provide and how. In addition, the framework identifies the support health workers need to deliver quality care and how education, regulation and an effective health care system contribute to building this support. In culmination of this research, a set of pragmatic steps for addressing the quality of SRMNH services has been created to facilitate moving from skilled care for some to quality maternal and newborn care for all.
Stay tuned for Petra’s follow-up blog on this topic next Tuesday, September 9th.