
Dr. Gene Declercq wants you to know three things about maternal mortality. But first, here are three things to know about him: (1) he eagerly pours over annual death certificate reports on weekend nights; (2) he maintains a slide with pictures of every colleague he’s published with, reminding us to join forces with others; and (3) he’s recently shifted his 30+ year research focus on childbirth to maternal mortality, because, as he states upfront, “regrettably death trumps birth in the eyes of the public.”
The United States ranks worse in maternal mortality than every other developed country. This ranking is fraught with international debate, measuring inconsistencies, and extreme racial inequities, especially among Black women in the U.S. During his presentation at the Harvard Chan School on April 6, 2018, Gene dug into all of these.
For instance, he quickly debunked the “diversity” argument that the U.S. ranks so poorly because of its diverse population and wide racial inequities in maternal mortality. Gene noted that even if we looked at maternal mortality just among White women, the U.S. still ranks at the very bottom. Thus, the U.S. is doing poorly by all standards — and racial inequities don’t explain the full picture.
With an ability to illuminate his findings with data sleuthing stories and memorable taglines, Gene gave us three things to know about the state of maternal mortality research in the United States:
- “The U.S. has a problem, but isn’t sure how bad it is.”
The main reason for this ambiguity is because of how maternal mortality is calculated in the U.S. compared to other countries. To set the stage, Gene spelled out the different maternal mortality measures the U.S. has used:
- Maternal mortality ratio – the death of a woman while pregnant or within 42 days of termination of pregnancy from any cause related to or aggravated by pregnancy or its management but not from accidental or incidental causes. Typically reported as a ratio per 100,000 live births.
- Pregnancy-related deaths – the death of a woman while pregnant or within one year of the end of pregnancy from a pregnancy complication, a chain of events initiated by pregnancy, or the aggravation of an unrelated condition of the physiologic effects of pregnancy.
- Pregnancy-associated deaths – the death of a woman while pregnant or within one year of termination of pregnancy, irrespective of cause. (Coincidentally, the World Health Organization calls these pregnancy-related deaths.)
In 2007, the U.S. federal government stopped reporting the maternal mortality ratio, the measure used by all other countries. Gene wanted to know why. In the U.S., the maternal mortality ratio had been increasing since the late 1990s. However, without newly reported maternal mortality data, we couldn’t make reliable comparisons to previous years or to other countries.
The answer, Gene and colleagues discovered, stemmed from the change in death certificate reporting in 2003. At the time, public health professionals worried that they weren’t picking up enough cases of maternal mortality during pregnancy. They sought to standardize how pregnancy information was collected on death certificates.
This led to the “pregnancy checkbox,” a mandated question on death certificates to indicate whether a deceased woman was pregnant or within one year of death. Unfortunately, the change required a huge technical overhaul, and when federal funding to support it fell through, states were slow to adopt. By 2007, maternal mortality data had become inconsistent with only half the 50 states (plus Washington D.C. and New York City) implementing the checkbox.
Give the checkbox debacle and fear of invalid data, the National Vital Statistics System (NVSS) decided to no longer report maternal mortality. The Pregnancy Mortality Surveillance System (PMSS) continued to report maternal deaths, but used different measures — pregnancy-associated deaths (deaths while pregnant or within one year of termination due to any cause) and pregnancy-related deaths (deaths while pregnant or within one year of termination associated with pregnancy) — instead of maternal mortality ratios.
That’s where Gene and his colleagues came in. They set out to analyze this inconsistent state data to estimate a national maternal mortality average, and once again, determine how the U.S. stacks up against other OECD countries. Their ensuing paper Recent increases in the US Maternal Mortality Rate – Disentangling trends from measurement issues, made waves when it was published in 2016. The article concluded that the estimated maternal mortality rate had increased by about 27% from 2000 to 2014 for 48 states and Washington D.C. (with California and Texas analyzed separately). The media had a field day, certain states reeled from the publicity, and soon there was an increased interest in the U.S.’s maternal mortality problem. Today, we’re still figuring out just how severe this problem is.
- “The problem is bigger than maternal mortality.”
Maternal mortality isn’t just about women dying in labor. It’s about what’s happening before delivery and after birth. It’s also what’s happening overall with increasing mortality rates for women of reproductive age, regardless of pregnancy status. Gene challenged us to broaden the conversation and our research.
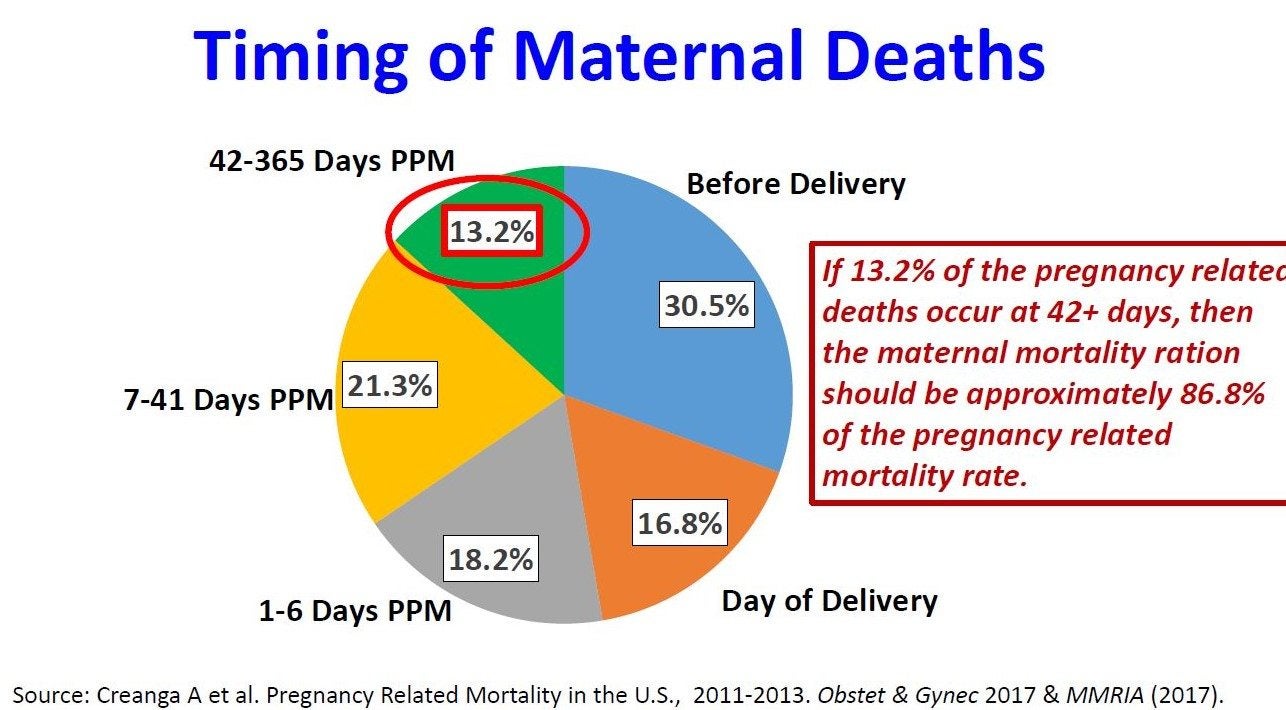
During his presentation, we learned that about 31% of maternal deaths happen before delivery and 33% after pregnancy (up to one year). The timing matters, specifically, the 12% of maternal deaths that occur between 42 days and one year after pregnancy since this range is not included in the maternal mortality ratio. This suggests that because the U.S. is using pregnancy-associated deaths and pregnancy-related deaths to measure maternal mortality, it is capturing more deaths in a wider time frame compared to other countries that use maternal mortality ratios as their measurement standards.
Gene also presented increasing mortality rates for young women, particularly those ages 25 to 34. The main cause for this increase? Accidents — a catch-all category encompassing mental health and accidental poisonings, including overdose deaths. With these findings, Gene has tapped into something much bigger than maternal mortality. And he calls on us to address it.
How can we as public health professionals expand our perspective of maternal mortality? How can we partner with fields like accidents and injuries to prevent women from dying? Part of the strategy lies in focusing more on pregnancy-related deaths and pregnancy-associated deaths.
- Re-conceptualizing maternal mortality and morbidity
Gene argued that maternal morbidity is a serious problem, too. Much progress has been made in clinical settings during birth, but cardiac issues, violence, and substance use during pregnancy are increasing.
Again, this requires us to see what’s going on before and after pregnancy or pregnancy termination. One way to do this is to ask women themselves. Their voices are critical to maternal morbidity research, but rarely captured in the data systems we have access to.
Gene wrapped up his seminar by reiterating needed solutions: listening to women directly, conducting longitudinal studies on maternal health, thinking beyond maternal mortality to women’s mortality overall, and shifting the narrative outside of hospitals. State maternal mortality review committees are starting to tackle these gaps by bringing together obstetricians, midwives, pregnant women, and researchers (Gene himself serves on the Massachusetts Maternal Mortality Review Committee).
As MCH stewards, we can learn from this approach. We can connect our detailed analyses to broader, more diverse issues. We can change the public image by prioritizing accurate data and compelling stories. And we can be collaborative and cross-cutting in our research.
There is no shortage of complexities when it comes to maternal mortality. With his three takeaways, Gene has given us a roadmap.
Dr. Gene Declercq is a Professor of Community Health Sciences and Assistant Dean for DrPH Education at the Boston University School of Public Health as well as a professor on the faculty of Obstetrics and Gynecology at the Boston University School of Medicine. Gene developed and presented the short film, Birth by the Numbers, as well as this companion website, which includes the specific data presented in this blog.